
Strength Training for Back Pain & A Strong Spine Health
Low back pain is incredibly common—about 80% of people experience it at least once in their lifetime.
In this article, we are going to review back pain basics, outline a model to help you better understand back and spine pain, and discuss how strength training can help to both improve and reduce the risk of back pain.
Despite its high prevalence, accurate information about low back pain—and what to do about it—can be hard to find. There are a lot of different - and scary - terms: “sciatica,” “herniations,” “bulges,” “stenosis,” “desiccation,” “radiculopathy,” and more. There are also countless treatment strategies that are, at best, confusing and, at worst, conflicting or incorrect: rest vs. exercise; stretching vs. no stretching; lift heavy weights vs. lift light weights; pelvic tilting; breathing; myofascial release; acupuncture; walking; meditation; specific supplements; injections; surgery—and so much more.
At EVOLVE, our physical therapists treat some type of low back pain almost every day. In almost every case, we find that people experiencing back pain are:
Confused about what is going on;
Scared that it will never get better
Tired of conflicting advice that gets them nowhere.
Does that sound like you, or someone you know? If so, read on.
Quick side note: While this article is primarily about low back pain (the most common type of spine pain), the same principles apply to the entire spine. There are some nuances when addressing neck or upper back pain vs. low back pain, but the overarching concepts are more similar than they are different.
Key takeaways
There are various types of low back pain. Identifying the exact anatomical structure causing pain is often difficult, and our treatment approach is typically similar regardless of the exact source of pain.
Advanced imaging, such as an MRI, is often unnecessary. Getting an MRI when you don’t need one can actually increase the risk of long-term pain and worse outcomes.
At EVOLVE, we’ve defined four key, research-supported pillars that contribute to low back health:
Mindset: Your beliefs about your low back—and the resilience of the spine (and entire body)—can affect how you feel and heal.
Systemic health: Low back pain is much more likely to occur, and to be longer lasting and more debilitating, when your body and mind are strained. Low back pain is affected by stress, mental health, nutrition, sleep, illness, and other factors that act on the body as a whole.
Movement patterns: How you move throughout the day, and during exercise, can significantly affect how your low back feels. Learning new ways of moving can be incredibly powerful.
Capacity: The lower back gets stronger in response to the right training. A stronger back, and stronger body overall, is less likely to be injured. Progressive exercise and strengthening can meaningfully reduce future low back pain episodes and recurrence.
Progressive loading is essential. Low-load exercises alone won’t build capacity in your lower back or system as a whole
Coached group strength training classes (like those offered at EVOLVE) may reduce the risk of low back pain recurrence because they assist with learning key movements, proper progression, and accountability/consistency.
Stretching and core drills can help, but long-term resilience usually requires whole-body strength, progressive loading, and coaching.
The goal isn’t to protect a fragile back. It’s to build a capable back.
My back hurts! What’s going on?
If your back hurts, the first thing to know is this: “back pain” is a symptom, not a single diagnosis. The low back is made up of several durable tissues that can get irritated in different ways, and many of the labels people hear (or see on an MRI report) don’t actually tell you what you need to do next. Let’s quickly ground you in the basics.
First, a quick anatomy tour. You don’t need to memorize these, but some common vocabulary can be helpful:
Vertebrae: The bones of your spine. Think of them like stacked building blocks designed to handle load and movement.
Disc (intervertebral disc): A specialized structure between the vertebrae that helps distribute force and allow movement. Discs are durable. A helpful comparison is that a disc behaves a bit like a specialized ligament (ligaments connect bone to bone). Discs can be irritated or injured, and they can also heal and adapt.
Facet joints: The small joints between vertebrae. Like any joint in the body (knee, knuckle, shoulder), they can become sensitive, stiff, or irritated—especially with certain positions or loads.
Foramen (intervertebral foramen): The openings on each side between vertebrae where nerves exit the spine.
Spinal canal: The central space that houses the spinal cord and other neural tissues.
Why many common “diagnostic” terms don’t actually help
A lot of low back pain labels sound specific, but they’re often used so broadly that they create more confusion than clarity. Here are some that you may have heard. Please note, we are including these to help you understand terms that you may have heard, or that are often used by other healthcare providers. We are not suggesting that you attach these labels to your symptoms. We’ll introduce a more useful framework later in the article.
Sciatica: Classically refers to nerve-related symptoms that travel down the leg (often below the knee), sometimes with tingling, numbness, or weakness. In everyday conversation, though, people use “sciatica” to describe everything from low back pain to butt pain to hamstring tendon irritation to true nerve pain. The word alone rarely tells us what’s actually driving your symptoms or what you should do about them.
Piriformis syndrome: Often used as a catch-all explanation for butt pain or in conjunction with “sciatica.” In reality, many different things can cause pain in the glute/hip region, and labeling it “piriformis syndrome” doesn’t automatically point to the right plan.
Disc bulge / disc herniation: These terms describe changes or injuries to the intervertebral disc. They can be relevant in some cases, especially when they clearly match a nerve-related symptom pattern. But they’re also commonly used like “sciatica” to describe almost any back pain. Perhaps most importantly, if an intervertebral disc is symptomatic, it can heal, often without surgery!
Stenosis: Refers to narrowing—either at the foramen (where nerves exit) or in the spinal canal. This term can matter, but it usually has a specific presentation that can be identified through a careful history and physical exam. Seeing the word on imaging doesn’t automatically explain your pain or predict your future.
Why an MRI often isn’t the first (or best) step
MRIs can be useful in the right situation, but they’re frequently ordered too early. The problem is that MRI reports often describe “findings” that are common in people who have no pain at all. When you’re hurting, it’s very easy to read the report and assume you’ve found “the cause,” even when the finding is incidental.
A few important MRI realities:
Many “scary-sounding” MRI findings are common in people with no pain at all, especially as we age. Dr. Bri likes to say, “I don’t look the same on the outside as I did when I was 18, and I probably don’t look the same on the inside either.”
Imaging findings often don’t predict how you function, how strong you can get, or whether you can return to lifting.
“Degenerative disc disease” is often a misleading, fear-provoking label for age-related changes that are frequently normal and not a life sentence of fragility. This term refers to loss of height of the intervertebral discs, and is commonly not associated with pain at all. Some healthcare organizations are pushing radiologists to stop using this term and instead label associated findings as “signs of normal aging.”
Research advises against getting an MRI in at least the first six weeks of a back pain episode in most cases.
In other words: an MRI can be a flashlight, but it’s not a map. The most useful “diagnostic” information usually comes from your story (how it started, what makes it better/worse) plus a physical exam and how your symptoms respond to movement and progressive loading.
When an MRI might actually be needed
There are situations where imaging is appropriate and important:
Red flags (serious symptom patterns): Serious spine pathology is rare, but does happen. If you have any of the following, don’t “train through it” – seek medical attention.
New bowel or bladder control problems
Numbness in the groin/saddle region
Progressive weakness in the leg or foot
Unexplained fever, chills, night sweats, or feeling systemically unwell
History of significant trauma with severe pain
Unexplained significant weight loss combined with severe persistent pain
Severe, unrelenting pain that doesn’t change with position or rest
Traumatic injury: Car accidents, falls from height, or other high-force trauma may require imaging to rule out serious injury or fractures.
Failure to improve with time and a good plan: If you’ve done consistent, appropriate rehab/physical therapy and meaningful progression for 3+ months without improvement, imaging may help clarify next steps.
Bottom line: Most back pain episodes are not dangerous, and most people can improve without immediately chasing a perfect label. The goal is to understand what category your pain likely fits into, reduce fear, and choose a plan that builds a more resilient back over time.
EVOLVE’s framework for low back pain
At EVOLVE, we don’t rely on a single “perfect diagnosis” to guide care—because for most people, low back pain is influenced by more than one factor. Instead, we use a framework that blends (1) a nuanced physical examination to rule in/out specific anatomical pain drivers and serious conditions, with (2) the bigger-picture variables that reliably influence whether back pain improves, recurs, or becomes persistent.
Physical therapy examination for lower back pain
Some cases of low back pain do have an anatomical source, or at least a specific pattern of symptoms, that we can identify with a nuanced and detailed physical therapy examination.
A physical exam is often more helpful than imaging early on because we can systematically test movement, positions, and specific tissues to see what reproduces symptoms and what reliably relieves them. That said, even with a nuanced exam, we don’t always get perfect clarity on the exact structure involved, and that’s okay.
Even when the “exact structure” remains unclear, our priorities with a physical exam are:
Ruling out serious pathology (anything that would require urgent medical evaluation; reference list above).
Identifying specific triggers—movement, positions, training habits, or lifestyle patterns that consistently flare symptoms.
Finding positions of relief and recovery that calm symptoms down and create space for healing (similar to elevating a sprained ankle to reduce symptoms and restore tolerance).
Video: Recovery position and relaxed breathing - We often recommend this position for 5-10 minutes, a few times per day, to patients who are currently experiencing high levels of back pain. It doesn’t solve everything, but it can help to calm things down. Of course, don’t persist with this if it worsens symptoms or doesn’t feel right.
Returning to movement and activity as soon as it’s appropriate, because relief positions are a short-term tool, not a long-term plan. We balance “calm it down” with “build it back up.”
The details of how we conduct physical examinations at EVOLVE are beyond the scope of this article. If you’re currently struggling with back pain, we recommend scheduling a physical therapy evaluation so we can explore your symptoms together.
That said, even a great physical exam has limits. Sometimes it helps us identify a likely pain driver, but it doesn’t automatically tell us the full solution. There are countless peer-reviewed studies on low back pain that discuss anatomy in detail, but offer few practical, meaningful next steps.
So, we need to go further than anatomy alone. And while we often recommend working with an experienced physical therapist, many people can make significant progress with the next part of our framework: the 4 Pillars of Low Back Health. These research-supported principles strongly influence how your low back feels and heals—and they provide a clear roadmap toward recovery.
Pillar 1: Mindset (beliefs, fear, expectations, and language)
Your beliefs about your back—what it is, what it can handle, and whether it can improve—have a real impact on pain and recovery.
Many people come to us after being told harmful, fear-provoking phrases like:
“You have the back of a 90-year-old.”
“Your spine is degenerating.”
“Your disc is slipping out.”
Even when a provider means well, language like this can create a powerful belief that your back is fragile and that normal activities are dangerous. That belief often leads to avoiding movement, bracing constantly, losing strength and confidence, and becoming more sensitive over time.
We emphasize a few key mindsets:
The body, and the spine, are resilient. They can adapt positively, build strength, and heal, at any age.
Expectations matter. Expecting something to hurt makes pain more likely. If you approach an activity convinced it’s dangerous, your nervous system is already on high alert.
Imaging does not tell the whole story. You don’t look the same on the outside as you did when you were 18, and you probably don’t on the inside, either—and that’s OK.
Complex problems are actually opportunities. A multitude of factors can contribute to low back pain—meaning we also have many therapeutic avenues to explore.
Our goal isn’t “positive thinking.” It’s accurate thinking: the spine is strong, adaptable, and built to move—and most backs can improve with the right approach.
Pillar 2: Systemic health (stress, sleep, habits, and the state of the whole person)
Low back pain is not just a “back problem.” It’s heavily influenced by the overall state of your body and nervous system.
When your body is strained overall, your pain sensitivity tends to increase and your recovery capacity tends to drop. This is a big reason why the same movement can feel fine one week and flare you the next.
Systemic factors that commonly influence low back pain include:
Stress load (work stress, life stress, emotional strain)
Sleep quality and consistency
Mental health (especially anxiety and depression)
Smoking
Alcohol intake
Low activity levels or prolonged sedentary time (for some people)
Malnutrition or low energy availability (not fueling enough to recover from life + training)
Illness and overall inflammatory load
Systemic health also affects how pain is processed. Research shows that pain is often felt to be more intense and longer-lasting when the nervous system and body are stressed. So, two people can have the same anatomical injury but experience it completely differently. This is another reason why MRI imaging—and even a physical examination—doesn’t tell the whole story.
Pillar 3: Capacity (strength, tolerance, and your “load ceiling”)
Capacity is your body’s ability to tolerate the demands you place on it—lifting, running, hiking, carrying kids, shoveling snow, or long work days.
Low back pain often shows up when demands exceed capacity. That can happen in three main ways:
Overloading: doing too much too soon, or a sudden spike in volume or intensity. Many active Flagstaff adults accidentally do this when their overall fitness is solid, but they jump into an activity with a lot of low back loading. They can “handle it” because of your athletic background—but the low back isn’t prepared for the specific exposure. Examples:
The seasons change and you ride 5 days in a row after a few months off the bike.
You push to finish a landscaping or home remodel project in one long weekend, putting in multiple 12-hour physically demanding days.
We get a big snowstorm and you shovel your driveway. Even a small driveway can mean a hundred (or more) shovel-loads of snow.
Underloading: avoiding movement and loading for long enough that your tolerance drops—so normal life demands become more consequential. Examples:
You had back pain and were told to rest. It helped a bit, but over a few months (or more), you lost strength and confidence.
Your partner hurt their back deadlifting, so you’ve avoided picking up anything heavy from the ground for years.
Life got busy and you haven’t been as active as you want. You finally try a fitness class, but leave feeling beat up and discouraged. It takes a few months to build up the resolve to go back, only to find things still hurt.
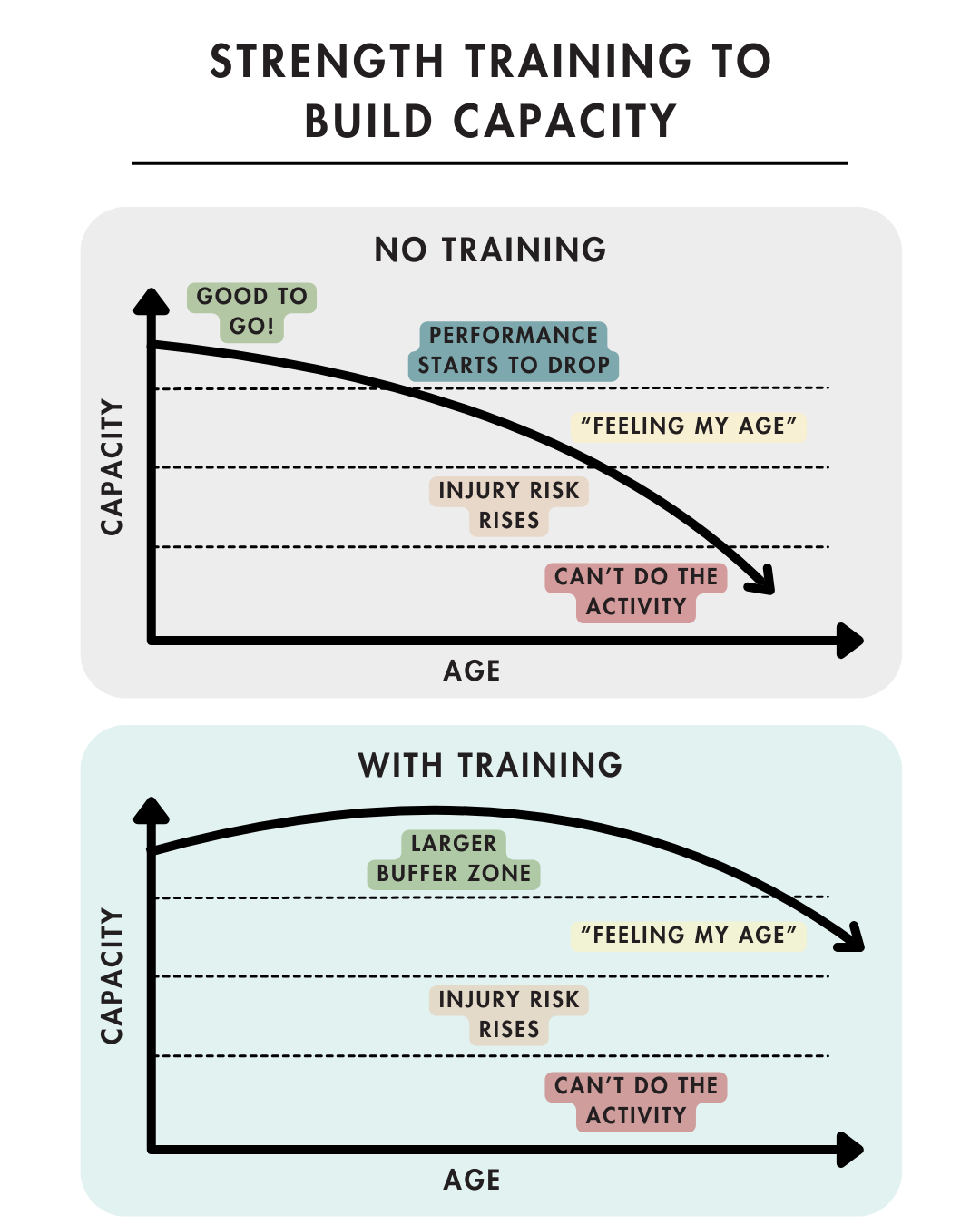
Getting older without strength training: Without strength training, the body will unfortunately lose capacity and strength as we age. This occurs even among endurance and outdoor athletes – these activities build cardiovascular fitness, but not specific strength. This results in tasks that used to be easy, feeling more challenging or risky. The good news? We can mitigate this decline with progressive strength training!
A useful way to think about this: the stronger you are, the less stressful everyday tasks become. If a heavy grocery load or a weekend project is close to your max, it’s easy to flare things up. If it’s only a small percentage of what you can handle, your back stays calmer.
How do we use an understanding of capacity to help lower back pain?
Assess loading patterns: were you overloaded or underloaded?
Build capacity! The more capacity you have, the less vulnerable your lower back, and entire system, will be
How do you build capacity? With progressive strength training! More on that below.
One key note: capacity is also influenced by systemic health. If you’re sleep-deprived, stressed, under-fueled, sick, or burnt out, your capacity drops—even if your “strength on paper” hasn’t changed. This makes it more likely that any given area of the body becomes painful.
Pillar 4: Movement Ability
Most of us were never taught how to move well. We learn to move as infants by watching our parents, and throughout life we pick up movement habits from sports, past injuries, repetitive jobs, and our environment.
Modern life is also relatively one-dimensional: we mostly move forward, and most built environments are flat. Even a Flagstaff local who spends a lot of time on trails still spends the majority of their time in modern built environments. All of these factors shape how we move. In particular, moving dynamically through the hips and the thoracic spine (mid/upper back) is challenging for many people—and the low back, caught between those regions, can end up overloaded as a result.
Additionally, pain changes how your brain and body perceive, process, and create movement. People in pain often move more rigidly, find it harder to monitor how they’re moving, and may struggle to change movement patterns. This is driven by a complex set of neurological changes in the systems that coordinate movement.
Put these together, and when someone has back pain it’s common to get “stuck” in patterns like:
Moving mostly through the low back instead of sharing the work with the hips and upper back
Avoiding certain directions entirely (like rotation), which can make those directions feel even more threatening over time
Bracing constantly, breathing shallowly, and losing fluidity
Moving slowly and cautiously, with less ability to move or react quickly
Lifting with a strategy that doesn’t distribute load well through the full system
When someone is in a high level of acute pain (“I just hurt my back for the first time”), these strategies may be temporarily protective. But they aren’t a long-term solution, and they can contribute to more pain and sensitivity over time.
The movement skills we commonly rebuild include:
Learning how to appropriately brace and use the core, and also how to relax it and breath deeply (the diaphragm has close connections to the lower back).
Hinging from the hips, rather than just using the knees or lower back.
Rotating from the hips and upper back (thoracic spine), not just the low back.
Moving fluidly and confidently in multiple directions and at different speeds: forward/backward, side-to-side, and rotation.
Handling load through the entire musculoskeletal system: legs, hips, trunk, shoulders, and arms
“Movement problem solving”—safely and progressively trying new or novel movements, and applying these concepts to them.
The goal is to give your body more options, distribute load more evenly, and restore confidence in real-world movement.
Summary of The 4 Pillars of Low Back Health
The key concept from these pillars: you don’t get hurt from load—you get hurt when load exceeds capacity. If we broaden our understanding of “load” and “capacity” to include not just physical efforts or actual heavy objects, we have a more nuanced, but also more helpful picture. How your lower back feels is related to:
Your mindset and beliefs
Your overall systemic health
Your overall capacity, relative to demands of your life and activities
Your movement ability
Strength training for recovery: why progressive loading works
For persistent or recurring low back pain, well-designed strength training helps because it:
Builds capacity and tolerance (so normal life loads feel less threatening)
Improves confidence with movement (reduces fear-avoidance)
Restores function (lifting, bending, carrying, walking, running, sports)
Stimulates a healing response in key tissues (the body heals itself in response to training!)
Improves quality of life by expanding what you can do reliably
Improves systemic health (sleep, stress, chronic disease risk factors, joint health, and more)
The key is progressive loading. If you’re currently in pain, we might start with light, gentle exercises to get you moving. But, as things calm down, a common back pain trap is staying forever in the “gentle” zone:
Light band work
Only stretching
Endless low-level core drills
Being careful forever
These activities can have a “shelf life” because they don’t prepare you for the true demands of life, and won’t stimulate the adaptations that promote healing and capacity.
Progressive loading means gradually increasing challenge over time:
More total work (sets/reps)
More resistance
More range of motion
More complexity and transfer to real-life movement
So, as symptoms calm down, you should look to gradually progress your strength training over time. We often see that individuals are “released” from physical therapy as their symptoms resolve, but before they truly progress to meaningful loading and strength training.
This is where a great strength program, or strength coach who is informed about low back pain, can be invaluable.
Why group exercise programs and classes can help
Supervised, group-based progressive strength training has shown better results than home exercise programs in at least one controlled trial for recurrence outcomes.
Why might group programs work so well?
Consistency (it’s scheduled; you show up)
Coaching (technique and pacing are supervised)
Progression (the plan is structured instead of random)
Confidence (you learn that loading is safe and helpful)
Community (adherence is better when you’re not doing it alone)
This is one of the biggest reasons EVOLVE Strong exists: coached group strength training is one of the best “containers” for doing the things that actually work—consistent practice and gradual progression.
What about the core? And stretching?
Stretching can help symptoms and can be part of a plan. But stretching alone usually doesn’t:
Raise your load tolerance
Improve your ability to lift/carry/twist confidently
Build durable trunk and hip capacity
Create a bigger buffer for unpredictable real-life demands
There are many reasons why muscles can feel tight (see article here) beyond just needing to stretch. In physical therapy, we might prescribe a stretch if there is a specific movement limitation that might be contributing to symptoms. However, general stretching typically doesn’t improve long term results.
And when it comes to core exercises: they matter, but they aren’t a magic solution for back pain. Core training can help you create stability around the spine, but your core isn’t meant to do all the work for real-life tasks. When you pick up something heavy, you need strong legs and hips to generate force, and strength in your upper back, shoulders, and arms to transfer and control that force. You’ll also feel better if you can hip hinge well.
Just as important: the goal isn’t to brace all day. Bracing is essential under load, but your trunk also needs to relax between efforts. Constant “holding tension” can be fatiguing and uncomfortable over time.
So at EVOLVE, we treat “core” like any other muscle group: we certainly include core exercises, but they shouldn’t dominate your entire program. The goal is a strong system.
When to start strength training vs when to see a PT first
If your back pain is in the past (not currently limiting you):
Start strength training with a good coach and a progressive program.
If your pain is mild (occasional ache/stiffness) and not limiting activity:
Start strength training with a good coach and a progressive program.
Click the button below to find the right strength program for you!
If your back hurts during or after exercise, or with daily movements:
Consider seeing a physical therapist first so you can identify triggers, build a tailored progression, and build confidence around movement and strengthening.
If your pain feels unpredictable (“anything might trigger it”) or you’ve stopped activities because you don’t trust your back:
See a PT first. Confidence and clarity matter, and a good plan can change everything.
How we help at EVOLVE Flagstaff
If you’re in Flagstaff and want a plan that builds long-term back resilience (not just temporary relief):
EVOLVE Strong: Coached group strength training built for long-term capacity and resilience
Foundations: Best if you’re returning after pain/injury or want technique coaching first
Personal Training: Individualized attention and movement coaching
Physical Therapy: If pain is limiting, persistent, or unpredictable
Registered Dietitian: Support your low back recovery and systemic health with appropriate nutrition and nourishment
Acupuncture: Reduce low back pain so that you can build capacity with training
References
Calatayud J, Cruz-Montecinos C, Casaña J, Guzmán-González B, Andersen LL, Morell MT, Roldán R, Ezzatvar Y. Effectiveness of a group-based progressive strength training in primary care to improve the recurrence of low back pain exacerbations and function: a randomised trial. Int J Environ Res Public Health. 2020;17(22):8326. doi:10.3390/ijerph17228326.
Chen J, Zhou R, Feng Y, Cheng L. Molecular mechanisms of exercise contributing to tissue regeneration. Signal Transduct Target Ther. 2022;7:383. doi:10.1038/s41392-022-01233-2.
Choi BKL, Verbeek JH, Tam WWS, Jiang JY. Exercises for prevention of recurrences of low-back pain. Cochrane Database Syst Rev. 2010;(1):CD006555. doi:10.1002/14651858.CD006555.pub2.
Cortell-Tormo JM, Tercedor Sánchez P, Chulvi-Medrano I, Tortosa-Martínez J, Manchado C, Llana-Belloch S. Effects of functional resistance training on fitness and quality of life in females with chronic nonspecific low-back pain. J Back Musculoskelet Rehabil. 2018;31(4):745-755. doi:10.3233/BMR-169684.
da Silva T, Mills K, Brown BT, Herbert RD, Maher CG, Hancock MJ. Risk of recurrence of low back pain: a systematic review. J Orthop Sports Phys Ther. 2017;47(5):305-313. doi:10.2519/jospt.2017.7415.
Falla D, Hodges PW. Individualized exercise interventions for spinal pain. Exerc Sport Sci Rev. 2017;45(2):105-115. doi:10.1249/JES.0000000000000103.
Gabbett TJ. How much? How fast? How soon? Three simple concepts for progressing training loads to minimize injury risk and enhance performance. J Orthop Sports Phys Ther. 2020;50(10):570-573. doi:10.2519/jospt.2020.9256.
Jackson JK, Shepherd TR, Kell RT. The influence of periodized resistance training on recreationally active males with chronic nonspecific low back pain. J Strength Cond Res. 2011;25(1):242-251. doi:10.1519/JSC.0b013e3181b2c83d.
Lee JS, Kang SJ. The effects of strength exercise and walking on lumbar function, pain level, and body composition in chronic back pain patients. J Exerc Rehabil. 2016;12(5):463-470. doi:10.12965/jer.1632650.325.
Maestroni L, Comfort P, Turner A, Read P, Bishop C, Papadopoulos K, Suchomel TJ. The benefits of strength training on musculoskeletal system health: practical applications for interdisciplinary care. Sports Med. 2020;50(8):1433-1450. doi:10.1007/s40279-020-01309-5.
Owen PJ, Miller CT, Mundell NL, Verswijveren SJJM, Tagliaferri SD, Brisby H, Bowe SJ, Belavy DL. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2020;54(21):1279-1287. doi:10.1136/bjsports-2019-100886.
Searle A, Spink M, Ho A, Chuter V. Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clin Rehabil. 2015;29(12):1155-1167. doi:10.1177/0269215515570379.
Steffens D, Maher CG, Pereira LSM, Stevens ML, Oliveira VC, Chapple M, Teixeira-Salmela LF, Hancock MJ. Prevention of low back pain: a systematic review and meta-analysis. JAMA Intern Med. 2016;176(2):199-208. doi:10.1001/jamainternmed.2015.7431.
Szczepaniak-Kucharska E. An analysis of the effectiveness of strengthening or stretching exercises in patients performing prolonged sedentary work with non-specific lower back pain. Ortop Traumatol Rehabil. 2024;26(3):57-68. doi:10.5604/01.3001.0054.7266.
Syroyid I, Cavero-Redondo I, Syroyid B. Effects of resistance training on pain control and physical function in older adults with low back pain: a systematic review with meta-analysis. J Geriatr Phys Ther. 2022;46(3):E113-E126. doi:10.1519/JPT.0000000000000374.
Wewege MA, Booth J, Parmenter BJ. Aerobic vs resistance exercise for chronic non-specific low back pain: a systematic review and meta-analysis. J Back Musculoskelet Rehabil. 2018;31(5):889-899. doi:10.3233/BMR-170920.
Welch N, Moran K, Antony J, Richter C, Marshall B, Coyle J, Falvey E, Franklyn-Miller A. The effects of a free-weight-based resistance training intervention on pain, squat biomechanics and MRI-defined lumbar fat infiltration and functional cross-sectional area in those with chronic low back pain. BMJ Open Sport Exerc Med. 2015;1(1):e000050. doi:10.1136/bmjsem-2015-000050.
Wong AYL, Karppinen J, Samartzis D. Low back pain in older adults: risk factors, management options and future directions. Scoliosis Spinal Disord. 2017;12:14. doi:10.1186/s13013-017-0121-3.